Surgeon Experience and Open Abdomen Management: Older and Wiser?
Author(s):
Jee Hwan Choi; Xian Luo-Owen; Steven Brooks; David Turay; Karen O’Bosky; Kaushik Mukherjee
Background:
Damage control has become the standard paradigm for patients with critical illness after trauma or intra-abdominal sepsis, and frequently results in temporary abdominal closure. Management of patients with an open abdomen is complex and has numerous ramifications, including prolonged mechanical ventilation and ICU length of stay and increased rate of intra-abdominal infections and fistulae. We studied the effect of attending surgeon experience on depth of sedation and paralytic use in patients with an open abdomen after trauma or emergency surgery.
Hypothesis:
We hypothesized that more experienced surgeons, as defined as having longer length of practice since their most recent fellowship or residency, would use deeper sedation and more frequently use paralytic agents to manage patients with an open abdomen.
Methods:
We performed an IRB-approved email survey of the senior and active membership in the Eastern Association for the Surgery of Trauma (EAST) using the Qualtrics application. The survey was sent to 1655 addresses, with a total of 393 responses(23.7% response rate). Data were analyzed using SPSS version 22.0 (IBM, Armonk NY) with Chi-square analysis for dichotomous outcomes and logistic regression to assess the effect of surgeon experience on sedation level.
Results:
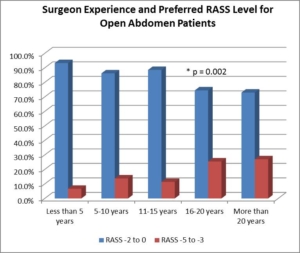
24.1%(n=94) of surgeons were less than 5 years, 25.6%(100) were 5-10 years, 18.7%(73) were 11-15 years, 12.3%(48) were 16-20 years, and 19.2%(75) were >20 years out from completion of training. Increasing surgeon experience was associated with deep sedation (RASS≤-3, p=0.002, Figure) and use of chemical paralysis (p=0.001) for open abdomen patients. Increasing surgeon experience was associated with less concern about delirium and more concern about evisceration as the reason for choice of sedation level (p=0.043) and more concern about evisceration as the reason for use of paralysis (p=0.001). After adjusting for fellowship training, trauma center level, and presence of trainees, surgeon experience was associated with increased likelihood of using deep sedation (p = 0.049, OR 3.6 [95%CI 1.3, 10.4]) for ≥20 years; OR 3.5 [95%CI 1.1, 10.4] for 15-20 years; NS for <15 years of experience).
Conclusions:
Surgeon experience is strongly associated with deep sedation and the use of chemical paralysis in patients with an open abdomen. Prospective data is necessary to validate these results and assess if an outcome difference exists, particularly with regard to infection and fistula.