
Role of Preoperative Antibiotic Treatment While Awaiting Appendectomy: The PERFECT-Antibiotics Randomized Clinical Trial
Reviewed by: Justin Dvorak, MD
Date of Review: November 2025
Title: Role of Preoperative Antibiotic Treatment While Awaiting Appendectomy: The PERFECT-Antibiotics Randomized Clinical Trial
Citation: Jalava K, Sallinen V, Lampela H, et al. Role of Preoperative Antibiotic Treatment While Awaiting Appendectomy: The PERFECT-Antibiotics Randomized Clinical Trial. JAMA Surg. 2025;160(7):745–754. doi:10.1001/jamasurg.2025.1212
Link to Article: https://pubmed.ncbi.nlm.nih.gov/40366704/
Context
Antibiotics are thought to decelerate inflammation progression and reduce complications in acute uncomplicated appendicitis. However, the effect of starting preoperative antibiotics on the appendiceal perforation rate is unclear. Due to this lack of clarity, considerable variation exists between hospitals and surgeons. The aim of the PERFECT-antibiotics trial is to determine whether it is safe to omit antibiotic treatment before appendectomy in acute, uncomplicated appendicitis.
Methods
Multicenter, open-label, non-inferiority randomized trial comparing antibiotic and no antibiotic treatment while awaiting appendectomy in adult patients with presumed uncomplicated acute appendicitis.
- Inclusion criteria: Adults with acute appendicitis scheduled to undergo appendectomy. Diagnosis was made clinically using the Adult Appendicitis Score, or via radiological imaging (U/S, CT, or MRI).
- Exclusion criteria: Pertinent exclusion criteria included pregnancy, need for immediate surgery, suspicion of complicated appendicitis, and known carrier of multi-resistant bacteria species.
Eligible patients were randomly allocated 1:1 to the antibiotic or no-antibiotic group. After randomization, patients in the antibiotic group were started on IV Cefuroxime 1500mg and IV Metronidazole 500 mg q8, while patients in the no-antibiotic group did not receive any antibiotics. Both groups received a single dose of prophylactic antibiotics (IV Cefuroxime 1500mg and Metronidazole 500mg) during anesthesia induction.
Primary outcome was perforated appendicitis. Pertinent secondary outcomes included duration of hospital stay, rate of conversion to open appendectomy, histopathological diagnosis of gangrene or perforation, post-op SSI, positive blood cultures up to 30 days post-randomization, and all 30-day complications.
A target size of 1800 patients was calculated based on anticipated rate of complicated appendicitis diagnosed intra-op of 15% and a non-inferiority margin of 5 percentage points, giving the trial a power of 90%, accounting for a drop-out rate of 3%.
Findings
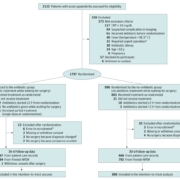
A total of 1,774 patients were included in the intention-to-treat analysis (888 in antibiotics group, 886 in no antibiotics group). Baseline demographics and clinical characteristics were similar between the two cohorts.
- Median age of the total cohort was 35, 1/3 of patients.
- Median in-hospital waiting time prior to surgery was 9 hours.
- The primary outcome of appendiceal perforation was detected in 74 patients in the antibiotic group (8.3%) and 79 patients in the no antibiotic group (8.9%) (0.6 percentage points, 95% CI -2.0 – 3.2 percentage points, p = 0.66).
- No antibiotics was non-inferior to antibiotics for progression to perforated appendicitis diagnosed intra-operatively.
- For the secondary outcomes, there were no differences in hospital stay, but the antibiotics group did have increased rates of SSI (3.2% vs 1.6%, p = 0.03) and increased positive blood cultures (0.9% vs 0.1%, p = 0.02). However, there was no difference in overall complications.
Commentary
In a multicenter randomized, non-inferiority clinical trial of adults with uncomplicated appendicitis, withholding pre-operative antibiotic treatment until surgery was noninferior to promptly starting antibiotics after diagnosis, for the progression to perforated appendicitis. There were also no differences noted in overall post-operative 30-day complications; however, the no-antibiotic group did have more SSIs and positive blood cultures. The rate of SSIs was low in both groups, with only 1% of patients in the no-antibiotic group requiring an intervention for SSI.
Implications
This study is well-done, and the results are interesting. The fact that post-operative SSIs were significantly increased for the no-antibiotic group does give one pause in terms of changing practice to withholding pre-operative antibiotic treatment. Increased post-operative infection was also higher in the per-protocol subgroup analysis. However, the differences in SSI were rather small and one could argue that it is not clinically significant.