Glutamine-Supplemented Parenteral Nutrition May be Associated with Increased Insulin Resistance in Surgical ICU Patients
Author(s):
Kaushik Mukherjee; Bryan Collier; Judith Jenkins; Kirk Easley; Thomas Ziegler; Addison May
Background:
Critical illness results in changes in glycemic control (GC) and insulin resistance (IR) that have been associated with increased infection and mortality rates. Small studies have indicated that parenteral nutrition supplemented with glutamine (GLN-PN) might reduce rates of infection and mortality. RCT’s have indicated that GLN might lower IR after trauma or critical illness. We performed a subset analysis of critically ill patients with dense GC data at a single surgical ICU after gastrointestinal, vascular, or cardiac surgery who required PN and were enrolled in the GLND multicenter RCT.
Hypothesis:
We hypothesized that GLN-PN would improve GC, decrease IR, and lower incidence of pneumonia compared to standard PN (STD-PN).
Methods:
This was a post hoc, single-center subset analysis of a cohort of patients enrolled in the GLND multicenter RCT of GLN-PN versus STD-PN in patients with a requirement for ≥7 days of PN and ICU care after gastrointestinal, vascular, or cardiac surgery. Patients were randomly assigned to receive either STD-PN or GLN-PN (isocaloric isonitrogenous PN supplemented with 0.5 g/kg/day glutamine dipeptide). Patients were followed daily with assessments for clinical outcomes and SOFA scores. Our cohort had dense GC data, comprising blood glucose (BG, mg/dL), insulin infusion rate (units/hr), and insulin multiplier M, a surrogate marker of insulin resistance utilized in a computerized glycemic control protocol.
Results:
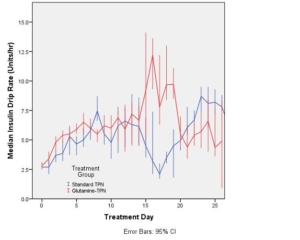
There were 20 patients in the STD-PN group and 21 in the GLN-PN group. Gender and mean age, body mass index, and APACHE II scores at study entry were comparable. Plasma glutamine and glutamate concentrations were higher in the GLN-PN group, as previously reported. There were no differences in the rates of hospital mortality and pneumonia between groups. There were no clinically significant differences in median daily BG or rates of hyperglycemia (BG>200) or moderate (BG<60) or severe (BG<40) hypoglycemia between groups. On days 2-6 and 17-20, the median daily insulin drip rate (Figure) and insulin multiplier M were higher in the GLN group (p <0.05).
Conclusions:
GLN-PN may be associated with increased IR as manifested by an increased insulin dose required to maintain euglycemia in critically ill post-surgical patients and increased insulin multiplier M.