
Risk of Surgical Site Infection in Exploratory Laparotomy
Author(s):
Erin Andrade; Jarot Guerra; Laurie Punch
Background:
Laparotomy incisions with contamination have higher incidence of surgical site infection (SSI). One management strategy has been to allow these wounds to heal by secondary intention to reduce rates of SSI; however, this results in ongoing need for wound care after discharge.
Hypothesis:
We hypothesized that the use of a high-risk incision closure protocol (HRICP) could allow for primary closure in contaminated wounds without increasing the SSI rate.
Methods:
A prospectively maintained Acute and Critical Care Surgery (ACCS) database spanning 2008-2018 was queried for patients who underwent exploratory laparotomy. Patients were stratified into two time periods 2008-2015 (no protocol) and 2016-2018 (closure protocol). All patients in the later period were operated on by a single surgeon utilizing HRICP, which included dilute Chlorhexidine lavage, closed suction drains for incisions deeper than 3 cm and topical negative pressure therapy. Trauma patients and in hospital deaths were excluded. CDC guidelines were used to determine wound classification and SSI based on chart review. Data were analyzed using chi-squared and logistic regression.
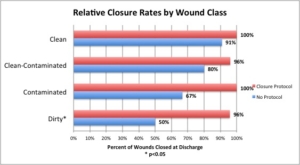
Results:
There were 148 patients who met study criteria. Rates of wound closure at discharge were higher in the closure protocol (CP) group than the no protocol (NP) group across wound classes but the difference only achieved significance in dirty wounds (50% NP vs 96% CP, p<0.0001). CP significantly increased the likelihood of wound closure at discharge (OR=42.9, p=0.001) even after controlling for age, gender, BMI, smoking, diabetes, and wound classification. The overall SSI rate, including superficial and deep space infections, was not significantly different in NP versus CP (18 vs 21%, p=0.659). Rate of superficial SSI was similar between NP and CP (10 vs 7.8%, p=0.653). In a subgroup analysis of contaminated and dirty wounds, CP increased the likelihood of wound closure at discharge significantly (OR=6869, p=0.015) and was not associated with increased risk of superficial SSI (OR=0.565, p=0.559) or overall SSI (OR=0.914, p=0.905).
Conclusions:
Utilization of HRICP allows for increased primary closure, less need for post-operative wound care, and a similar rate of SSI. Further study of the components of HRICP are required to assess which ones have maximal impact in minimizing SSI after high-risk closure.