
Reintubation does not Increase Pneumonia Rates when Controlled for Ventilator Time
Author(s):
Jessica Weaver; Andrew Young; Jason Saucier; Patrick Reilly; Carrie Sims
Background:
Reintubation in the intensive care unit (ICU) is a common occurrence and is associated with increased rates of pneumonia, longer hospital stays and increased mortality in multiple studies. However, it is not clear whether this increased morbidity comes from the reintubation itself, or the result of a longer ventilator course.
Hypothesis:
We hypothesized that when ventilator time was controlled for, complications rates would be the same in both groups.
Methods:
All patients intubated in the trauma ICU between 1/1/2012 and 6/30/2018 were considered for this retrospective case-control series. Patients intubated within 48 hours of extubation were considered “reintubated,” and a total of 164 reintubated patients were found. Patients were matched for exact number of ventilator days, gender, blunt versus penetrating injury, ISS range, and age within 10 years. Sixty-eight patient pairs were identified. Odds ratios were calculated using SPSS (IBM).
Results:
After matching by total number of ventilator days (average 7.3 days in both groups), the reintubated and not reintubated groups were similar, including percent female (both 16.2 %), age (48.5±21.0 vs 47.8±21.3), and ISS (22.3 vs 21.7). Complications were equivalent between groups other than a higher rate of substance withdrawal among the reintubated patients. Reintubation was associated with a lower mortality (OR 0.12, CI 0.03-0.43).
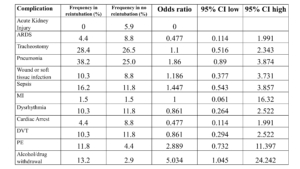
Conclusions:
When patients were matched for total ventilator time, reintubation was not associated with increased pneumonia or other complications. This suggests that risk of pneumonia is due to the increased ventilator time rather than the reintubation itself. Unexpectedly, mortality was also significantly decreased in the reintubation group, though further study is needed to understand the mechanism behind this difference. Our findings suggest that our fears associated with “failed extubation” may be exaggerated, a more aggressive extubation strategy may be beneficial.