
High Tidal Volume Ventilation is Associated with Ventilator-Associated Pneumonia in Acute Cervical Spinal Cord Injury
Author(s):
Gabrielle Hatton; Patrick Mollett; Shuyan Wei; Radha Korupolu; Sasha Adams; Charles Wade; Lillian Kao
Background:
Respiratory complications are the main cause of morbidity and mortality after acute spinal cord injury (SCI). Complications are attributed to hypoventilation, increased respiratory secretions, and impaired cough. High tidal volume ventilation (HVtV) is used in SCI rehabilitation centers to overcome hypoventilation while weaning from the ventilator. The effect of HVtV on respiratory complications such as ventilator-associated pneumonia (VAP) during the acute post-injury period is unknown.
Hypothesis:
SCI patients receiving HVtV in the acute post-injury period is associated with lower incidence of VAP when compared to patients receiving standard tidal volumes.
Methods:
This was a cohort study of adult (>16 years) trauma patients with cervical SCI admitted to a level 1 trauma center from 2011 to 2015. Exclusion criteria included: head abbreviated injury scale >5, mechanical ventilation <2 days, and a diagnosis of acute respiratory distress syndrome. HVtV was defined as a median tidal volume >10cc/kg ideal body weight during time on ventilator up to two weeks post-injury. VAP was defined according to the National Trauma Data Base Dictionary. Univariate, multivariable, and Bayesian analysis using a neutral prior were utilized to interpret the data.
Results:
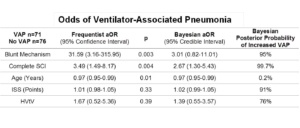
Of 147 patients included, 71 (48%) developed VAP. HVtV was utilized in 20 (14%) patients. Demographics were similar between patients who received HVtV and standard ventilation, except patients were younger in the HVtV group. VAP developed in 70% of patients receiving HVtV and in 45% receiving standard tidal volumes (p=0.01). After adjustment, HVtV resulted in an odds ratio of 1.39 for VAP, credible interval 0.55-3.57, and a posterior probability of 76% that HVtV increases pneumonia (Table).
Conclusions:
This is the first study to evaluate the association between HVtV and VAP in the acute post-injury period. While limited by small sample size and selection bias, our data did not reveal benefit from HVtV for patients with cervical SCI in the acute post-injury period, contrary to findings during the rehabilitation period. Further investigation into optimal early ventilation settings is needed for SCI patients, who are at a high risk of VAP.