
Catheter-Associated Urinary Tract Infections Among Trauma Patients: Poor Quality of Care or Marker of Effective Rescue?
Author(s):
Husayn Ladhani; Esther Tseng; Jeffrey Claridge; Christopher Towe; Vanessa Ho
Background:
Catheter-associated urinary tract infections (CAUTI) are a widely-used quality indicator, prompting significant resource allocation towards prevention. Although CAUTI is known to be generally associated with poor outcomes, the effect of CAUTI on specific clinical outcomes is poorly described in trauma patients.
Hypothesis:
We hypothesized that trauma patients with CAUTI would have worse outcomes such as prolonged length of stay (LOS), discharge to a facility, and death.
Methods:
Patients with LOS >2 days in the 2016 Trauma Quality Improvement Program database were included. Patients with and without CAUTI were matched 1:1 via a propensity score using patient, hospital, and injury factors, including injury mechanism, abbreviated injury scores, and comorbidities (caliper 0.05, no replacements). Outcomes were compared between matched pairs, including other hospital acquired infections (HAI), LOS, intensive care unit (ICU) LOS, ventilator days, unplanned events (intubation, operation, and ICU admission), discharge disposition, and mortality, using the Wilcoxon matched-pairs signed rank test for continuous and exact McNemar test for categorical variables.
Results:
The incidence of CAUTI was 0.73%. 1,529 matched pairs were created from a cohort of 246,126 patients. Propensity match effectively reduced bias; post-match propensity score variables all had absolute standardized differences <0.1. In matched pair analysis, CAUTI patients had lower mortality compared to patients without CAUTI (7.1% vs. 10.9%, p<0.05). CAUTI was associated with higher rates of other HAIs, longer overall and ICU LOS, more ventilator days, more unplanned events, and fewer discharges home (all p<0.01, Table).
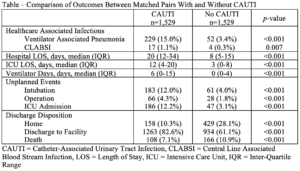
Conclusions:
Trauma patients with CAUTI had improved survival despite higher rates of other HAIs, longer LOS, more ventilator days, and fewer discharges to home. The CAUTI group had more unplanned events perhaps suggestive of interventions intended to prevent mortality after complications, such as ICU admission, intubations, and operations. Therefore, CAUTI may be a consequence of effective “rescue” care that leads to decreased mortality, rather than a marker of poor quality.