
Temporal Profile of the Inflammatory Response During Six-month Follow Up After Severe Trauma
Author(s):
Lauren Kelly; Jennifer Munley; Erick Pons; Kolenkode Kannan; Philip Efron; Alicia Mohr
Background:
Post-discharge inflammation and its correlation with recovery following severe trauma is poorly described. Severe traumatic injury induces a systemic inflammatory and hypercatecholamine response associated with critical illness and end organ dysfunction, including disordered hematopoiesis and anemia. This study sought to characterize trajectory and resolution of the postinjury inflammatory state.
Hypothesis:
We hypothesized that severe trauma would induce prolonged inflammation lasting several months after injury.
Methods:
This single-institution cohort study prospectively enrolled 90 trauma patients with an injury severity score >15, hemorrhagic shock, and a pelvic, hip, or femur fracture. Patients undergoing elective hip replacement (n=34) were enrolled as operative controls. Plasma was obtained at enrollment and after 14 days, one, three and six months. Inflammatory cytokines were measured using immunosorbent assays. Cytokines at each time were compared using two-tailed t-tests with correction for multiple comparisons in GraphPad Prism v9.1.
Results:
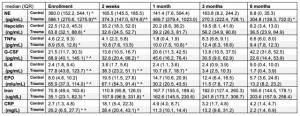
Plasma levels of norepinephrine (NE), hepcidin, C-reactive protein (CRP), interleukin (IL)-6, granulocyte colony stimulating factor (G-CSF), tumor necrosis factor alpha (TNFa) and erythropoietin were significantly elevated on enrollment compared to operative controls (Table 1, presented as median (IQR), * adjusted p value < 0.05, ^ clinically elevated). Erythropoietin, G-CSF, TNFa, and CRP were elevated following trauma for two weeks. IL-6 was persistently elevated compared to controls for up to 1 month. NE remained elevated and significantly higher than controls at 2 weeks, and this elevation was again significant at 6 months. Using a multiple linear regression model, there was a significant relationship (R2 = 0.312) between day 14 IL-6 and hospital length of stay (p = 0.03) and total red blood cell transfusions (p = 0.03).
Conclusions:
Severe trauma is associated with a persistent inflammatory and hypercatecholamine response. This inflammatory response in turn is associated with increased transfusion requirements and prolonged hospitalization. Further analysis is needed to identify correlations between persistent inflammation and clinical outcomes after discharge.