Neonatal SOFA Scores Predict Mortality in Infants with Necrotizing Enterocolitis and Spontaneous Intestinal Perforation
Author(s):
Irving Zamora; Marshall Wallace; Jamie R. Robinson; Mhd Wael Alrifai; Joern-Hendrik Weitkamp; Stephanie Moore; Jon Schoenecker; Shilin Zhao; Ashley E. Markowski; Jeffrey Upperman; Martin Blakely
Background:
Necrotizing enterocolitis (NEC) and spontaneous intestinal perforation (SIP) are common conditions affecting premature infants, which typically lead to sepsis, very unpredictable clinical courses, and high rates of infectious morbidity and mortality. In adults the Sequential Organ Failure Assessment (SOFA) predicts mortality. Similarly, neonatal SOFA (nSOFA) scores have been shown to predict mortality in infants with sepsis. Investigators have not evaluated whether nSOFA scores predict mortality in infants with NEC and SIP.
Hypothesis:
We hypothesized that repeated nSOFA scores, automatically embedded within the electronic medical record, would predict mortality in neonates with medical or surgical NEC and SIP.
Methods:
A retrospective, single-center study of preterm neonates admitted between 2019 and 2022. The nSOFA scores were analyzed for patients with NEC and SIP for the 72 hours surrounding surgical consultation and surgical intervention.
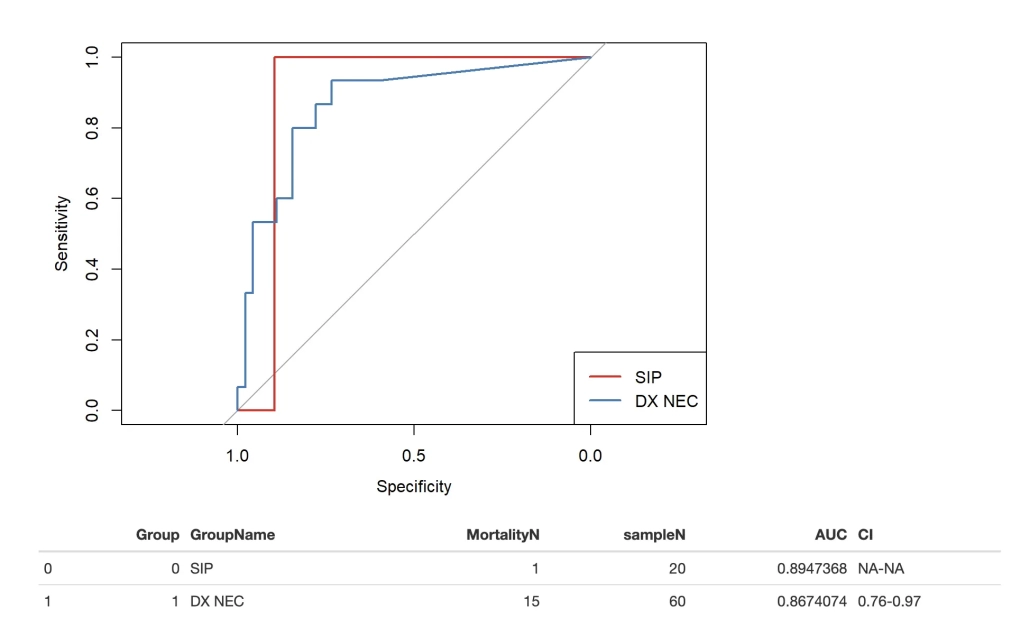
Results:
In the 80 infants who met inclusion criteria, 60 (75%) had NEC, and 20 (25%) had SIP. Of the NEC patients, 53 (88%) had medical NEC and 7 (12%) had surgical NEC. Overall mortality was 20% (n=16). Mortality rates were: 85% (6/7) in surgical NEC, 17% (9/53) with medical NEC, and 5% (1/20) with SIP. Surgical intervention was performed in 36 (45%) patients; 21 had peritoneal drain placement and 15 had laparotomy. Receiver operating characteristics area under the curve for mortality (Figure 1) was 0.87 (95% CI: 0.76–0.97) for NEC and 0.89 for SIP patients around the time of surgical consultation, demonstrating a strong association of nSOFA score and mortality. Independent of diagnosis, nSOFA scores prior to intervention were also different between survivors and non-survivors (Figure 2).