Open versus Laparoscopic Appendectomy: A post hoc analysis of the EAST Appendicitis MUSTANG Study
Author(s):
Lauren Thompson; Brianna Cohen; D. Yeh, MD; Walter Ramsey; Patricia Byers; Nicholas Namias; Jonathan Meizoso
Background:
We sought to understand which factors are predictive of open appendectomy as final operative approach.
Hypothesis:
We hypothesize that higher American Association for the Surgery of Trauma (AAST) Emergency General Surgery (EGS) grade is associated with open appendectomy.
Methods:
Post hoc analysis of the EAST MUSTANG prospective appendicitis database. All adults undergoing appendectomy were stratified by final operative approach: laparoscopic or open appendectomy (including conversion from laparoscopic). Univariate analysis was performed to compare group characteristics and outcomes, and multivariate logistic regression was performed to identify demographic, clinical, or radiologic predictors of open appendectomy.
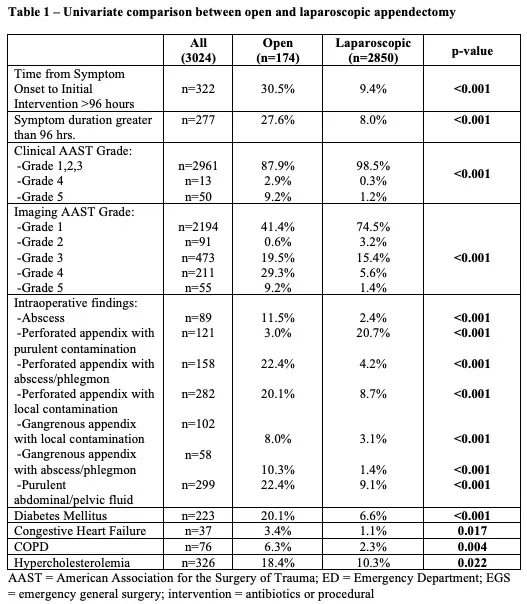
Results:
3024 cases were analyzed. 174 (5.8%) patients underwent open appendectomy, including 116 converted from laparoscopic to open. Mean age was 41±16 y and 53% were male. Compared to the laparoscopic group, open surgery was associated with more comorbidities; higher proportion of symptoms greater than 96 hours; higher AAST EGS grade; and higher incidence of perforated and gangrenous appendicitis with purulent contamination, abscess/phlegmon, and purulent abdominal/pelvic fluid on intraoperative findings (Table 1). On multivariate analysis controlling for comorbidities, clinical and imaging AAST grade, duration of symptoms, and intraoperative findings, only AAST Clinical Grade 5 appendicitis predicted open appendectomy (OR 6.12, 95% CI 1.32-28.34, p=0.02).
Conclusions:
In the setting of appendicitis, only generalized peritonitis (AAST Clinical Grade 5) on presentation was associated with increased odds of open appendectomy.