
Effect of Depth of Surgical Site Infection on Mortality in ICU Patients
Author(s):
Christopher Towe, Nathaly Llore, Nathalie Hirsch, Jessica Donington, Harvey Pass, Vanessa Ho, NYU Langone Medical Center
Background: Empyema can result as a complication of bacterial pneumonia or thoracic surgery procedures with mortality as high as 15%. Empyema pathogens are poorly described in the modern era. Greater understanding of common pathogens and risk factors is aAuthor(s):
Caitlyn Cookenmaster; Tjasa Hranjec; Robert Sawyer
Background:
Surgical site infections (SSIs) can be classified into superficial incisional (skin and subcutaneous tissue), deep incisional (fascia and muscle), or organ space infections and are presumed to be caused by microbial contamination of one or more of these depths. Deeper infections are thought to result in worse patient outcomes.
Hypothesis:
We hypothesize that SSIs may be indicators of immunoincompetence or pathobiomic hostility with superficial incisional infections being associated with improved survival.
Methods:
A retrospective cohort study of 643 ICU patients treated for SSI at two institutions from 1997-2023 was performed. Demographics for the three groups—superficial incisional (SI), deep incisional (DI), and organ space (OS)—were compared using univariate analysis with multiple comparisons. Logistic regression was used to evaluate risk factors associated with mortality.
Results:
104 SI, 275 DI, and 264 OS infections were identified. For all infections, mean age was 57.2 ± 0.6 years, APACHE II score was 18.4 ± 0.3, and length of stay was 31.1 ± 1.3 days. Enterococcus and Candida species were the most common isolates, but were significantly more frequent in the deeper SSIs (DI and OS). Crude mortality was similar between the three groups: 28.9% in SI, 22.9% in DI, and 19.7% in OS. The most important predictors of mortality were presence of liver disease, trauma, and SSI. When adjusted for risk factors, superficial incisional SSI was independently associated with higher mortality. (Table 1)
Table 1. Risk factors for mortality in ICU patients with surgical site infections.
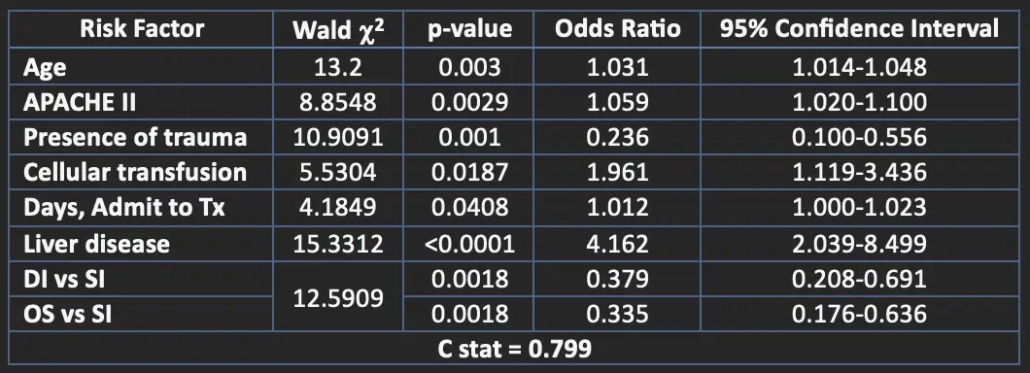
Conclusions:
Among critically ill patients, superficial incisional SSIs are associated with higher mortality when compared to deep incisional or organ space SSIs. These results suggest that the pathogenesis of an SSI event may be more of an indicator of immunoincompetence or a hostile pathobiome, rather than a simple contamination event. More basic science research focusing on the molecular, immunological, and microbial aspects of surgical site infections is required.
required to improve empiric treatment. The primary aim of this study is to describe the microbiology of empyema in the modern era.
Hypothesis: We hypothesize that parapneumonic empyema (PNE) and post-surgical empyema (PSE) will be clinically and microbiologically distinct.
Methods: All patients with positive pleural cultures between 4/2007 and 6/2012 were identified from microbiological records. Patient demographics, clinical course and microbiological information were collected. Each acute empyema was classified as PNE or PSE and differences between groups were assessed using the Chi-square test.
Results: A total of 227 microorganisms from 28 genus classes were isolated from 125 patients (74 (64%) male, mean age 61). 120 (97%) required drainage and/or decortication, while 5 were treated with antibiotics alone. Common comorbidities included: a history of immunosuppression (29%), diabetes (19%), and renal disease (14%). Mortality was 15%. Half (47.7%) of the index cultures were polymicrobial. 152 isolates (67%) were gram positive, 56 (25%) were gram negative, 16 (7%) were fungal, and 3 (1%) were unclassified. Only 7% of isolates were obligate anaerobes. The most common organisms were Streptococcus spp (27%) and Staphylococcus spp (25%), followed by Enterococcus spp (9%), Candida (6%), and Pseudomonas (6%). Of 31 isolates of S. aureus, 14 (45%) were methicillin resistant. 29% of the infections were postoperative. Patients with PSE were less likely to have had a preceding pneumonia (28% vs 65%, p<0.05). Patients with PSE had a slightly higher incidence of gram-negative pathogens but this did not reach statistical significance (40% vs 26%, p=0.1). There was no difference in outcome between the PNE and PSE patients.
Conclusions: A wide variety of pathogens were isolated from infected pleural cultures. The most common pathogens isolated were aerobes and gram positives. Polymicrobial infections were common. There was no significant difference in clinical course or pathogens isolated from parapneumonic and post-surgical empyema.