Author(s):
Elizabeth Krebs; Shayan Rakhit; Jennifer Beavers; Leanne Atchison; Robel Beyene
Background:
Our trauma center initiated a protocol for de-escalation of empiric vancomycin in patients with a negative methicillin resistant staphylococcus aureus (MRSA) nasal swab in June 2022. However, in March 2023 our institution subsequently implemented a hospital-wide policy of admission nasal mupirocin MRSA decolonization which hindered the reliability of MRSA nasal swabs and prevented their use for de-escalation.
Hypothesis:
We hypothesized that the hospital-wide MRSA mupirocin decolonization practice would have the unintended consequence of prohibiting the nasal swab based de-escalation protocol and be associated with increased vancomycin use.
Methods:
This retrospective review evaluated all patients admitted to a Level 1 trauma center, comparing those admitted during the de-escalation (“de-esc”) and decolonization (and thus “no de-esc”) protocols. The primary outcome was total days of vancomycin per patient receiving vancomycin, with associations measured with linear regression. Additional outcomes included proportion of patients receiving fewer than 3 days of vancomycin, overall vancomycin rates, and in-hospital MRSA infections, with associations measured with logistic regression.
Results:
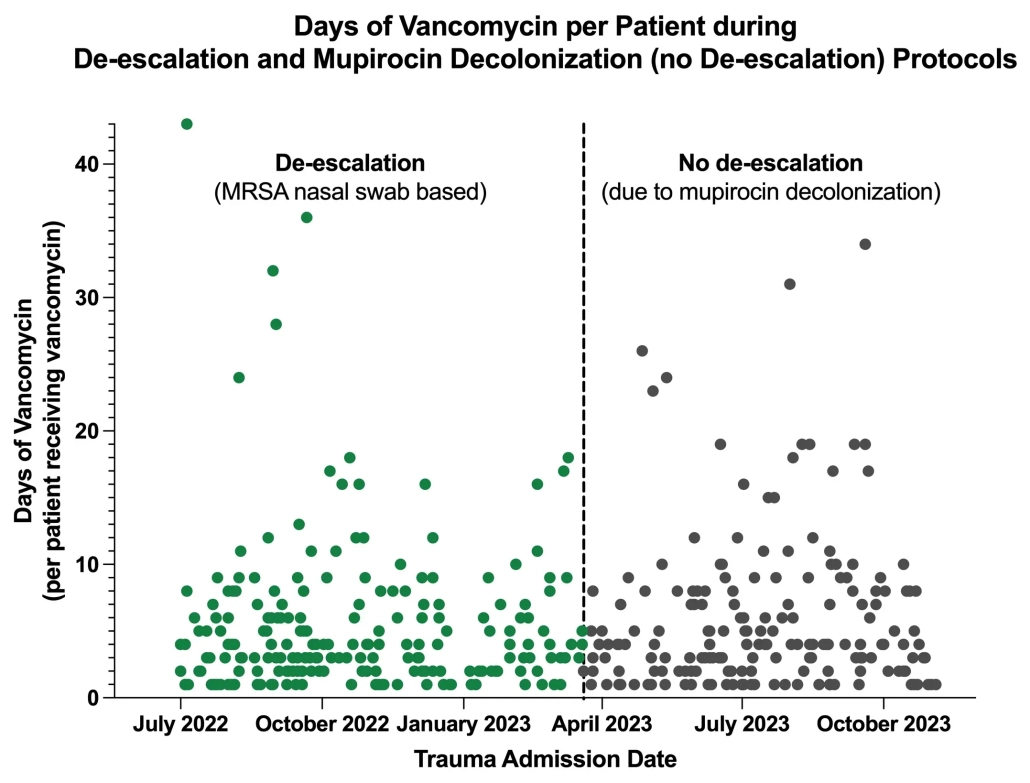
A total of 5678 patients were admitted during the time period, with no difference in proportion of patients receiving vancomycin during the “de-esc” vs. “no de-esc” protocols (7.2% (n=208) vs 6.5% (n=181), p=0.3). The distribution of days of vancomycin prescribed vs. admission date is shown in Figure 1. Amongst these patients, there was no difference in either total days of vancomycin (5.3 days vs 5.9, p=0.3) or proportion receiving fewer than 3 days of vancomycin (33% vs. 29%, p=0.5) between the groups. There were 56 total patients with MRSA infections, with no difference during between the “de-esc” and “no de-esc” protocols ).
Conclusions:
Contrary to our hypothesis, when unable to use an MRSA nasal swab based de-escalation strategy due to universal mupirocin decolonization, de-escalation rates remained high with no significant increase in vancomycin use. This demonstrates the value of pharmacist involvement and institutional culture towards promoting antibiotic stewardship.
Figure 1: