Clinical Synergism: Combined Fungal and Bacterial Intra-Abdominal Infections Associated with Increased Mortality
Author(s):
Elizabeth Krebs; Taryn Hassinger; Zachary Dietch; Nathan Elwood; Kimberly Ann Popovsky; Robert Sawyer; Traci Hedrick
Background:
Multiple synergistic interactions have been identified between fungi and bacteria, including co-aggregation into mixed biofilms, enhanced growth via signaling molecules, and shared metabolic byproducts. However, the clinical implications of these interactions are largely unknown. While fungal and bacterial co-infection is common in complicated intra-abdominal infections (IAI), outcomes from combined infection have not been well studied.
Hypothesis:
We hypothesized that synergistic interactions between fungus and bacteria would lead to higher mortality in patients with combined IAI.
Methods:
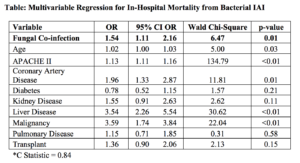
All surgical patients admitted to a single academic institution between 1996 and 2014 were queried for presence of a culture-proven bacterial IAI. Univariate analyses compared characteristics between patients with a combined fungal and bacterial IAI and those with bacterial IAI alone. Multivariable logistic regression evaluated the effect of fungal presence in IAI on in-hospital mortality, while controlling for APACHE II score and select comorbidities. A subgroup analysis evaluated unadjusted mortality rates for common fungal-bacterial combinations.
Results:
Of 1887 patients with culture-proven bacterial IAI, 503 (26.7%) were co-infected with fungi. Patients with a fungal component were older (57.0 vs. 55.5 years, p=0.025) with a higher median APACHE II score (15 vs 13, p < 0.01) but without differences in trauma or transplant status or comorbidities including diabetes, coronary artery disease, liver disease or kidney disease. The most common bacterial pathogens were Enterococcus spp. (25.6%), E. coli (16.9%) and Streptococcus spp. (12.0%). The most common fungal pathogens were Candida albicans (40.4%) and Candida glabrata (24.9%.) The presence of fungal species was associated with increased crude in-hospital mortality (16.9% vs. 9.8%, p<0.01), and on multivariable regression, fungal co-infection remained associated with death (Table). The highest mortalities were associated with fungal co-infection with Enterobacter spp. (28.6%), Enterococcus spp. (28.3%), and P. aeruginosa (26.3%).
Conclusions:
We identified an association between fungal presence and in-hospital mortality in patients with bacterial IAI. Continued research into cross-kingdom synergistic relationships will identify potential therapeutic targets in the management of IAI.