
Complications after Duodenal Injury: Too Much Resuscitation?
Author(s):
Vanessa Arientyl; Victoria Wagner; Alejandro De Leon; Jonathan Nguyen; Randi N. Smith; Chris Dente; Elizabeth Benjamin; S Rob Todd; Jason Sciarretta
Background:
Duodenal trauma is a rare and potentially life-threatening injury. There is sparse literature investigating the impact of perioperative resuscitation volume or composition on duodenal complications post repair.
Hypothesis:
We hypothesize that higher volumes of crystalloid during the perioperative phase (first 24 hours of presentation) will increase the risk of duodenal leak (DL) and other complications.
Methods:
A retrospective cohort review of 57,489 patients between January 2012-June 2023 was performed. Patients with traumatic duodenal injuries requiring operative repair were included. Demographics, operative details, injury grade, hospital length of stay, ventilator days, complications, 24-hour blood transfusion volume (BTV), 24-hour crystalloid fluid volume (CFV) and 24-hour total resuscitation volume (TRV = BTV + CFV) administration records were collected.
Results:
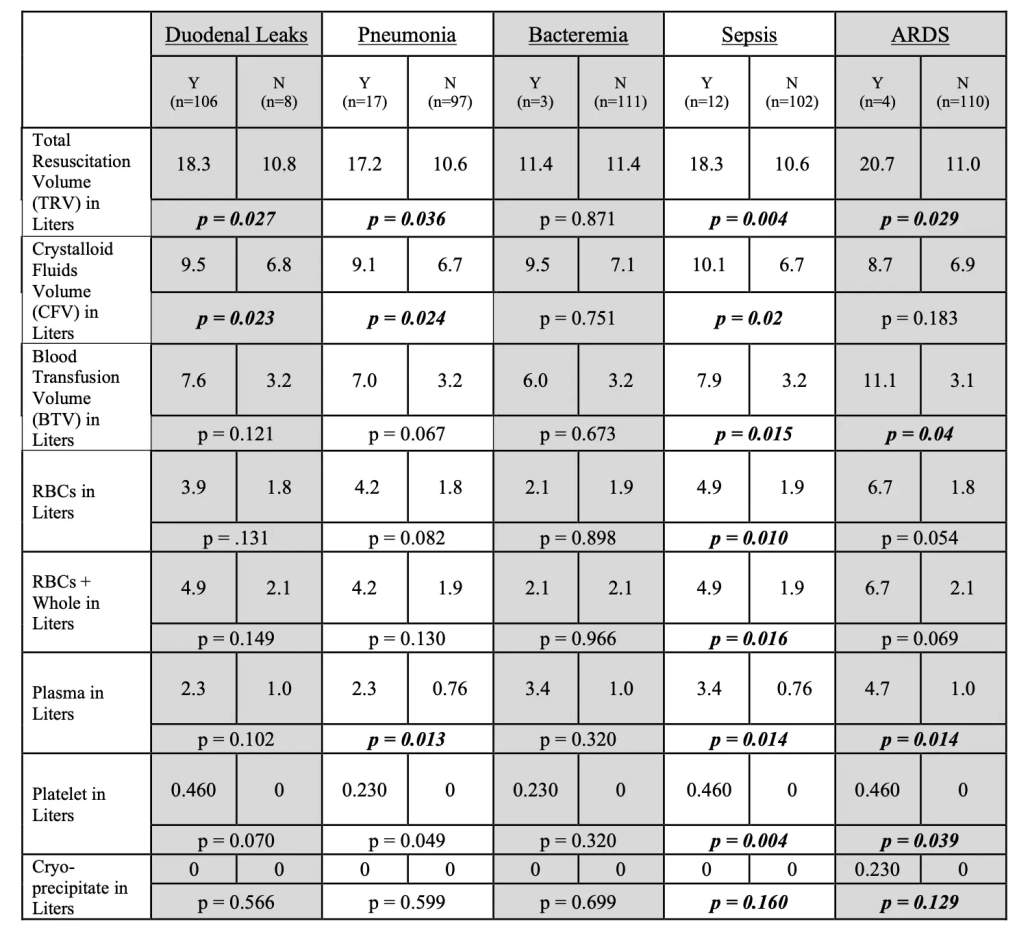
114 patients comprised the cohort. Median (IQR) age was 28.5 (22-38) years, with 81% males, the majority penetrating (87%), and a median ISS of 25 (16-29). Of these patients, 8 developed a DL. Those with a DL had higher CFV (6.8L v 7.1L) and TRV (10.8L v 18.3L). The 17 patients who developed pneumonia also received higher CFV, plasma and TRV. There was no association with the CFV, BTV or TRV received in those who developed bacteremia. The development of ARDS was not associated with the CFV, but rather BTV and TRV. ARDS was also associated specifically with plasma, cryoprecipitate and platelet volume. In regard to the development of sepsis, CFV, BTV and TRV were all associated with increased rates. Of note, this association was also seen with higher volumes of the individual blood components (RBC, plasma, cryoprecipitate and platelets). Using binary logistics regression, CFV in 24 hours was contributory to the development of DL (p=0.041), sepsis (p=0.006), and pneumonia (p=0.039) while the BTV was associated with the development of ARDS (p<0.001).
Conclusions:
Our data suggests perioperative resuscitation may significantly impact complications such as duodenal leak, pneumonia, sepsis and ARDS in patients with duodenal trauma. Patients who with higher crystalloid and total resuscitation volume perioperatively are at increased risk of duodenal leak, pneumonia and sepsis, while those who receive a large volume of blood products are at increased risk of developing sepsis and ARDS.