Fever and Trauma are Protective in ICU-Acquired Infections
Author(s):
Nathan Elwood; Taryn Hassinger; Zachary Dietch; Elizabeth Krebs; Kimberly Ann Popovsky; Traci Hedrick; Robert Sawyer
Background:
Patients admitted to the ICU with a primary diagnosis of trauma are known to have better survival from ICU-acquired infections compared to non-trauma surgical patients. Victims of trauma are also more likely to be febrile during infection, perhaps due to an ischemia-reperfusion-induced enhancement of the immune response.
Hypothesis:
We hypothesized that the survival benefit seen with a traumatic diagnosis among surgical patients with ICU-acquired infections is due to a greater incidence and degree of fever associated with a more robust immune response.
Methods:
All patients admitted to the surgical and trauma ICUs at a single academic institution from November 1996 to July 2014 were prospectively surveyed for the development of ICU-acquired infection. A retrospective cohort study was conducted comparing in-hospital mortality between trauma and non-trauma patients with and without fever. Univariate analyses assessed patient and infection characteristics and multivariable logistic regression adjusting for clinically relevant concurrent effects was used to identify predictors of in-hospital mortality, particularly the interplay between fever and trauma status.
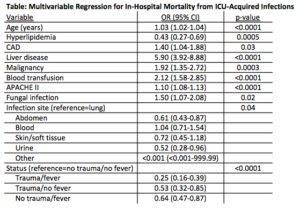
Results:
We identified 941 trauma patients and 1449 non-trauma patients with ICU-acquired infections. The most common site of infection was lung (31%) followed by abdomen (29%). Trauma patients were younger (48 vs. 59, p<0.001), less likely to be female (27% vs. 44%, p<0.001), more likely to receive transfusion (74% vs. 47%, p<0.001), and had lower APACHE II scores (18 vs. 19, p=0.02). Trauma patients were more likely to have fever (72% vs. 43%, p<0.001), with a higher maximum temperature (38.8 vs. 38.2, p<0.001), and had lower in-hospital mortality (9.6% vs. 22.6%, p<0.001). In multivariate analysis, when compared to non-trauma patients without fever (Table), trauma patients with fever had the lowest mortality (OR 0.25, p<0.001). Trauma patients without fever and non-trauma patients with fever also had lower mortality (OR 0.53 and 0.64, both p<0.001).
Conclusions:
Both an admitting diagnosis of trauma and the presence of fever are associated with better survival after ICU-acquired infection. The traumatic state itself may activate a systemic response that is protective in subsequent infections; however, since afebrile trauma patients also have improved survival, this trauma-mediated survival benefit appears to be dependent on other mechanisms in addition to fever.