
Non-operative Management of Cholecystitis in Pregnant Patients Remains Common
Author(s):
Jessica Weaver; Alan Smith; Todd Costantini; Laura Haines
Background:
Cholecystectomy is the recommended treatment for acute cholecystitis in pregnancy, leading to fewer pregnancy-related complications than non-operative management (NOM). However, past research demonstrated high rates of non-operative management despite these recommendations. Rates of cholecystostomy tube usage and outcomes in pregnancy are not well-described.
Hypothesis:
We hypothesized that rates of interventions for cholecystitis have increased.
Methods:
The National Readmissions Database (NRD) was queried for all visits in the first 3 quarters of each year 2016 to 2019, that included a patient with an ICD-10 code for cholecystitis or pregnancy. These entries were then further investigated for demographics, gestation, rates of interventions at the index admission (cholecystectomy or cholecystostomy tube), 90-day readmissions, interventions at readmission, and pregnancy-related complications.
Results:
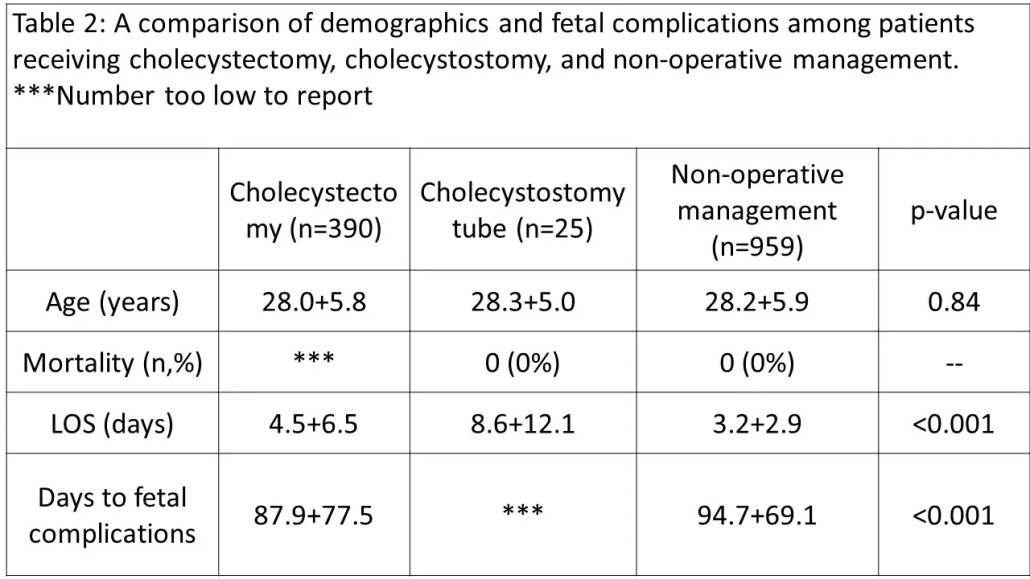
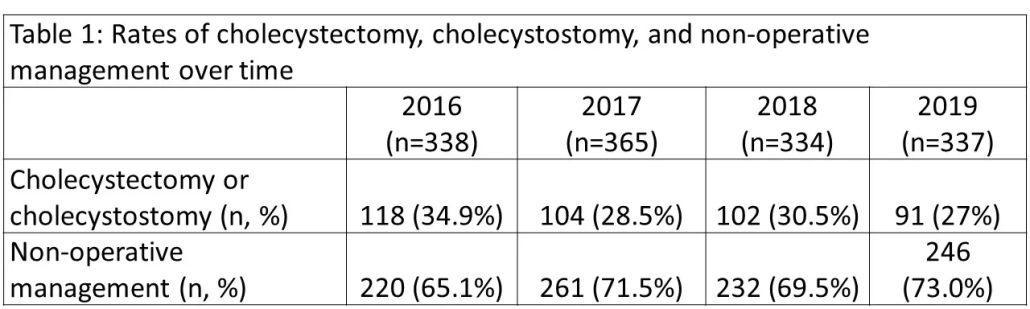
Annual rates of interventions for cholecystitis remained low over the study period, p=0.135 (Table 1). There were 4.62% of patient who require readmission for cholecystectomy. Compared to the 1st trimester, interventions were more likely in the second trimester (RR 1.88 CI 1.32-2.66, p<0.001) and less likely in the 3rd trimester (RR 0.20 CI 0.14-0.27, p<0.001). Length of stay was highest for cholecystostomy tube placement and lowest for patients that received NOM.
Conclusions:
Cholecystectomy rates in pregnancy remain low despite evidence that cholecystectomy is safe. Cholecystostomy appears to be a safe alternative, but associated with a longer length of stay. Further study is needed to determine what barriers exist to adequate treatment of cholecystitis in pregnant patients.