Nosocomial Infections in Trauma Patients Receiving ECMO
Author(s):
Larisa Shagabayeva; Luciana Tito Bustillos; Megan Laurendeau; Jessica Delamater; Michael Cobler-Lichter; Nicole Lyons; Brianna L. Collie; Oswald Perkins; Edward Lineen; Valerie Hart; Jonathan P. Meizoso; Tiago Machuca; Nicholas Namias; Kenneth G Proctor; Brandon Parker
Background:
The utility of extracorporeal membrane oxygenation (ECMO) in acute trauma patients is growing, but the risk of infection in this demographic has not been well defined.
Hypothesis:
This study aims to characterize the infections in trauma patients while receiving ECMO.
Methods:
All trauma patients (n=50) who required ECMO at a level 1 trauma center between 2014 and 2023 were retrospectively reviewed. All blood and respiratory samples collected during each patient’s hospital stay were examined for pathogens. Burn injuries were excluded from this study.
Results:
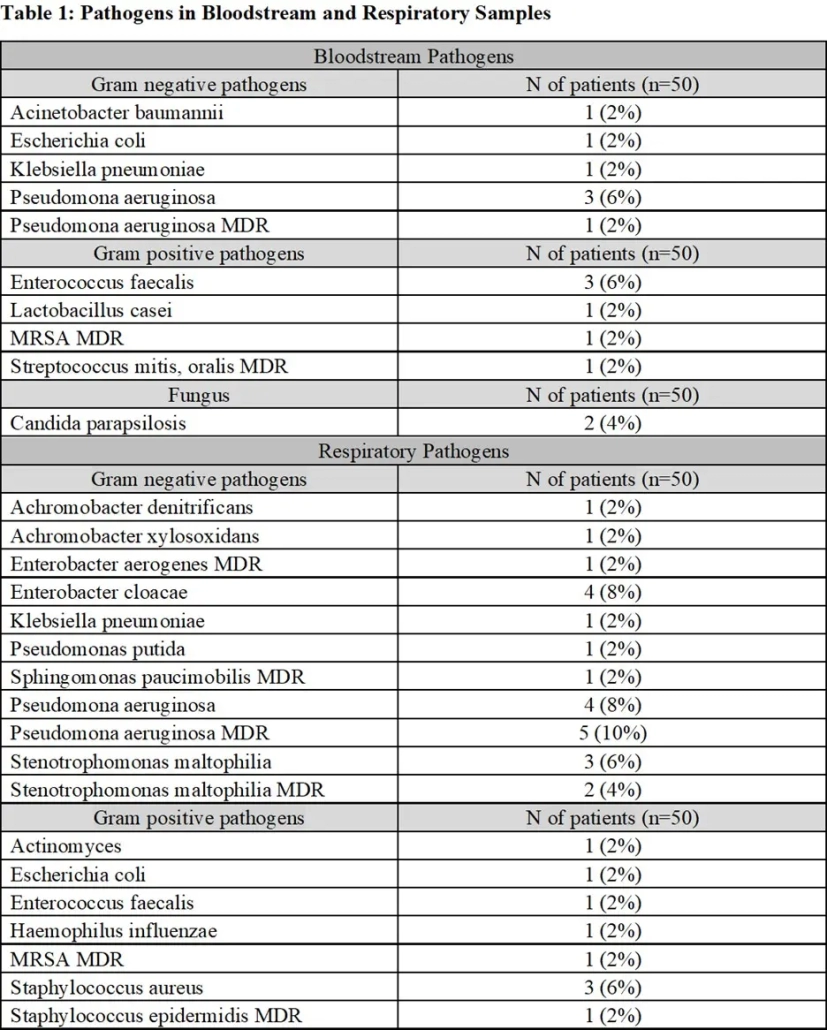
Of all 50 trauma patients identified, most were male (88%) who sustained blunt injuries (60%), of which the most common mechanism was motor vehicle collision (37%). The median ICU length of stay was 25.5 days (IQR:12.25-53.50), median ventilator days was 21.5 (IQR: 8.5-50.8) and median length of ECMO treatment was 8.0 days (IQR: 4.0-18.0). The most common ECMO type was VV (70%), however 6 patients required multiple ECMO modalities. Bloodstream and/or respiratory infections were detected in 22 (44%) patients, which is no different from a 45% infection rate in trauma patients in the ICU reported on existing literature (p=0.873). In our sample, the most common was respiratory infection (73%). Gram negative pathogens were most common in both bloodstream (47%) and respiratory infections (79%). Among the bloodstream pathogens, 20% were multi-drug resistant. Among the respiratory pathogens, 30% were multi-drug resistant. The most common location of ECMO cannulation in patients with bloodstream infections was at the ICU bedside (62%), and of these, 60% were bifemoral cannulations. The median number of days from ECMO cannulation to bloodstream infection was 8.0 days (IQR 3.8-16.0) and the median number of days to respiratory infection was 7.0 days (IQR: 7.0-10.3).
Conclusions:
Nosocomial infections, particularly respiratory, are prevalent among trauma patients receiving ECMO. Although infection rates are not statistically different between ECMO trauma and ICU trauma patients, routine cultures to detect early infections in trauma patients receiving ECMO may be advisable given the unique challenges associated with ECMO.