
Pneumonia Mortality in General Surgery Patients Vs Solid Organ Transplant Patients
Author(s):
Jose Lopez-Vera; Robert Sawyer
Background:
Pneumonia continues to be a common and morbid infection, and is the 3rdmost common postoperative complication in surgical patients, leading to significant increases in length of stay, cost, morbidity, and mortality. Unlike non-trauma general surgical patients, transplant patients have a unique disadvantage in that the host immune response to grafts, the “alloresponse,” as well as chronic immunosuppressive therapies put them more at risk for pneumonias and other infections.
Hypothesis:
We hypothesized that while comparing pneumonia between general surgery and solid organ transplant patients and controlling for the presence of immunosuppression, the presence of the alloresponse would be an independent predictor of poor outcomes.
Methods:
We analyzed prospectively collected data from all non-trauma general surgery patients and transplant patients from 1997 – 2017 treated for pneumonia at a single institution. Demographics and outcomes including mortality, days of treatment, and length of stay were compared. We used Student’s t-test to compare continuous variables and chi-square analysis for categorical variables. Multivariable logistic regression analysis including age, APACHE II, WBC, Tmax, time from admission to antibiotics, ventilator dependency, liver disease, immunosuppression, and the presence of a solid organ transplant was used to determine independent predictors of mortality.
Results:
During the study period, 1293 patients with pneumonia were treated, including 316 with transplants and 977 treated on the general surgery services. The following demographic variables were significantly different between transplant patients and non-transplant patients: age, APACHE II, WBC, Tmax, days from admission to antibiotics, ventilator dependency, liver disease, immunosuppression, and healthcare-associated disease. Duration of antibiotic therapy was longer in the transplant group (18.6 ±1.4 versus 13.2 ±0.5 days, p < 0.0001), but crude mortality was similar (25.9 versus 25.8%). Logistic Regression results shown.
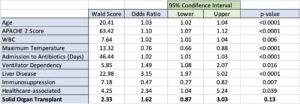
Conclusions:
Compared to general surgery patients treated for pneumonia, transplant patients have significant differences in demographics. However, when controlled for severity of illness, the presence of immunosuppressive therapy, and other variables, organ transplantation was not a risk factor for death. The presence of a transplanted organ and the related immune activity of the alloresponse do not appear to worsen the response to infection.