
Primary and Secondary Empyema have distinct bacterial pathogens: implications for empiric antibiotic treatment
Author(s):
Christopher Towe; Sudershan Srinivasan; Vanessa Ho; Malavika Kesavan; Katherine Wu; Stephanie G. Worrell; Yaron Perry; Philip Linden
Background:
Empyema can be characterized as either primary (parapneumonic) or secondary (post-traumatic, perforation, or procedure), and often requires surgical intervention.
Hypothesis:
We hypothesized primary and secondary empyema have distinct bacteriology.
Methods:
Consecutive surgical decortications in an academic Medical Center from 1/1/2010-10/1/2017 were reviewed and categorized as primary or secondary empyema. Cases were matched to microbiology cultures. Descriptive statistics were used to describe the relationship of cultured bacteria to empyema type.
Results:
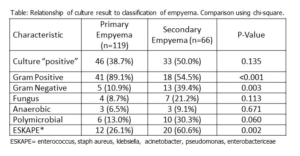
183 patients were included; 119 (64%) had primary and 66 (36%) had secondary empyema. Positive culture results were present in 79 (43%), 46/119 (38%) with primary empyema and 33/66 (50%) with secondary empyema (p=0.14). The most commonly isolate was Streptococcus, present in 29 (37%), followed by Staphylococcus in 19 (24%). 11 patients (13.9%) had fungal infections. 16 (20%) patients had polymicrobial empyema.
Primary and secondary empyema differed in several ways (table), including the rate of gram-positive and gram-negative isolates, and specifically the presence of ESKAPE pathogens (Enterococcus, S. aureus, Klebsiella, Acinetobacter, Pseudomonas, Enterobactericeae). There was a trend towards higher rates of fungal infections in secondary empyema, candida infections were more common in secondary empyema (2/46 vs 7/21, p=0.02).
Streptococcus species rarely exhibited resistance (7% intermediate to ceftriaxone, 4% intermediate to PCN). Staph Aureus was frequently resistant (26% clindamycin, 25% ciprofloxacin, 89% to penicillin, 42% to oxacillin (MRSA), and 5% to TMP-SMX). Seven MRSA isolates were tested against carbapenems and were resistant to imipenem, meropenem, and ertapenem. All MRSA were susceptible to linezolid and vancomycin.
Conclusions:
Distinct bacteriology characterizes primary and secondary empyema, which may support individualized empiric antibiotic treatment for empyema based on etiology. Multi-institution study to establish antibiotic guidelines for empiric treatment prior to surgical culture and drainage is appropriate.