
Wide Variation in Prophylactic Antibiotics for Operative Isolated Traumatic Facial Fractures
Author(s):
Mandi Roberts; Angela Sauaia; Ernest Moore; D. Yeh, MD
Background:
The role of prophylactic antibiotics in adults undergoing operative fixation of facial fractures remains unclear and is not supported by the current Surgical Infection Society guidelines. The purpose of this study was to document current practice patterns and determine the event rate of infectious complications during index hospitalization.
Hypothesis:
We hypothesize there will be a wide variation in practice and a low incidence of infectious complications.
Methods:
The 2019-2021 TQIP was queried for isolated facial fractures (upper face, midface, or mandible) requiring operative interventions. Adults (≥ 18y) from facilities with ≥ 10 cases were included. Prophylactic antibiotics were defined as any antibiotics received prior to the start of operative fixation. Clinical endpoints were infection-related complications, defined as deep surgical site infections (SSI), organ space infections, osteomyelitis, sepsis, and superficial incisional infections. Major infections were defined as deep SSI, organ space infections, osteomyelitis, and sepsis.
Results:
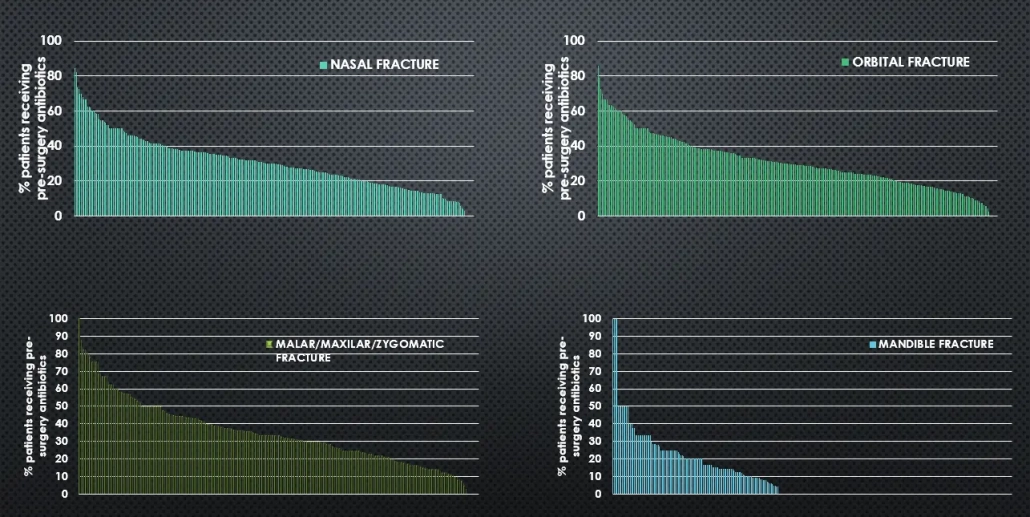
There were 10,680 patients in 312 facilities with 3069 (29%) receiving prophylactic antibiotics. The incidence of major infections was 0.1% (n=13) and any infection was 0.2% (n=20). There was wide variation in practice, with centers ranging from 3% to 79% of patients receiving prophylactic antibiotics (Figure 1). This was seen across all fracture types including nasal, orbital, mandible and maxilla/zygomatic fractures. When comparing highest vs. lowest quintile of % antibiotics, there were no statistically significant differences between hospitals regarding verification level, bed size, teaching facility status, or hospital type.
Conclusions:
There is wide variation in the practice of administering prophylactic antibiotics to trauma patients with isolated facial fractures requiring operative intervention. The incidence of infections is extremely low during the index admission. Long term outcomes are required to detect clinically significant infectious complications. This study establishes clinical equipoise; thus a randomized controlled study with an innovative design to overcome the low incidence of complications is warranted to inform this practice